Given the critical importance of improving maternal and child health, quality of care and access to ANC to reduce newborn and maternal mortality; IHF has now ventured into an innovation partnership under the “Empowering Mothers with Birth Readiness, Agency, and Care” (EMBRACE) programme. EMBRACE offers a compelling model for how partnerships can transform maternal and child health outcomes in low- and middle-income countries. At its core is a powerful collaboration between a philanthropic anchor focussed on maternal and child health with extensive presence in India and Africa, where IHF will now apply its proven model of supporting innovation development for public health challenges to identify potential approaches to develop affordable, minimally and non-invasive diagnostics and pregnancy management tools for use in primary care in low resource settings.
Over the next three years, IHF will build a structured pipeline of solutions in a set of maternal focused priority areas (Figure), supporting mid to late-stage solutions through product development, clinical and operational validation, and evidence generation; with
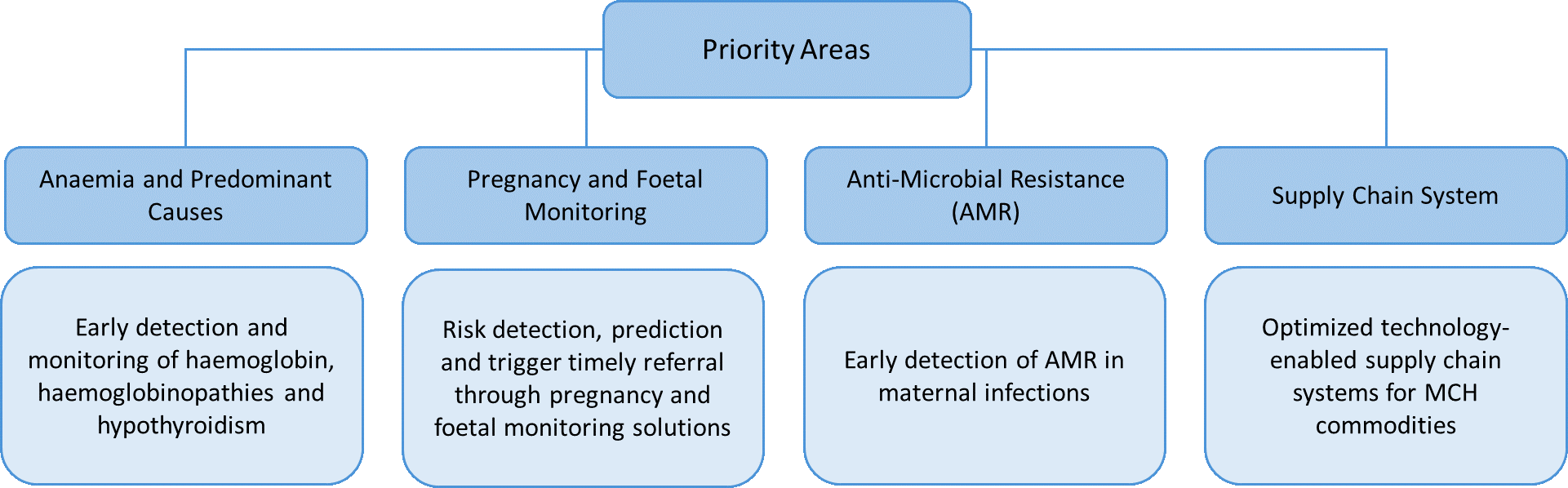
deployment through local implementation partners who bring critical contextual knowledge and ensure last-mile delivery. The areas of focus will be expanded or modified as the initiative develops and can also be adapted to meet the specific innovation requirements of partners. This approach will bridge the evidence to adoption gap for science-based innovations in maternal health by embedding innovations into service delivery models, supply chains and clinical practice.